
- ippocrateios@sopi.it
"BUTTERFLY
TIP"
- OPERATION:
- SURGICAL
TECHNIQUE
-
- LIONELLO
PONTI, M.D.
-
- During the last three decades various
authors have emphasized the importance of a meticulous reshaping
of the alar cartilages in rhinoplasty, if a good cosmetic and
functional result is to be obtained. The initial Joseph technique
has been modified in various ways and new techniques have been
added to it.
- Many of the methods involve reduction of
the width, length and height of the alar cartilages by resection
of a segment along the superior edge of the lateral crus, and
another at the level of the dome, so that the resected part is
hockey-stick shaped. Excision of the alar cartilages, if performed
correctly, produces good remodelling of the nasal tip.
- For many years, we have been using the
Goldman technique, which we have modified to avoid certain
pitfalls. The reduction of the alar cartilages and the remodelling
of the tip is entirely different in our technique.
- Surgery of the tip is usually the most
delicate and difficult part in a rhinoplasty. This technique makes
reshaping of the alar cartilages simpler and more precise, so that
the outcome of the operation is more predictable.
-
- OPERATIVE
TECHNIQUE
-
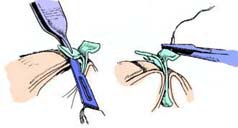
- When correction of the upper two-thirds
of the nose has been completed, a semicircular marginal incision
is made. It extends from the upper third of the columella, along
the inferior edge of the alar catilage, to the lateral end of the
lateral crus . A small curved pair of scissors is inserted into
the incision, a plane of cleavage is found under the perichondrium
and the overlying soft tissues are undermined, by opening the
scissors .



-
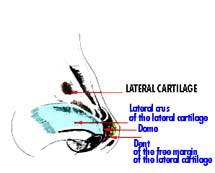
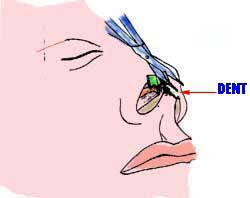
- The undermining and dissection are
extended to the intercartilaginous incision and in between the
medial crura. Once the alar cartilage has been freed, it is pulled
down with a hook applied at the level of the dome and brought into
direct view . At the junction between the medial and the lateral
crura, it is possible to identify a dent which is very important
for this kind of method.
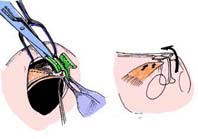
- A grooved hook is placed under the dome
to serve as a guide, and the junction between the lateral and the
medial crura is cut through, a few millimeters lateral to the
dent. This incision is limited to the cartilaginous layer alone,
the underlying vestibular skin being left intact The same
procedure is repeated on the other side. The medial crura are
hooked together and exposed through the right nostril. These are
pulled and sutured together with a mattress suture.
- The-placement of this suture is
extremely important because it determines the projection and shape
of the tip.

-
-
- If the medial crura are not
well-aligned, the tip of the nose will be deformed. That is why it
is important to have a reference point for the suture: this point
is the dent, and the suture will be placed at the same level as
the dent, or immediately below, or above it.
-
- In this way, a pillar will be formed by
the medial crura topped by two small wings of cartilage
corresponding to portions of the dome.
- It is the shape of this structure which
led us to call this technique the "butterfly tip".
-
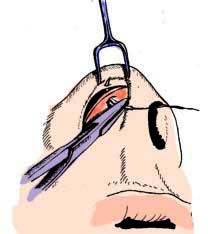
- Once the projection and length of the
tip have been established, we reduce the length and the height of
the lateral crura if necessary so that they match the medial crura
. After placing them in situ, the surgeon palpates the tip and, if
necessary, proceeds to the free margins of the medial crura ). The
lateral crura are reduced by excising a segment along the superior
edge, and another along the portion lateral to the dome
.

- Finally, any remaining irregularity or
defect is corrected by additional resections, as
indicated.
- Before the patient leaves the table, the
tip is re-evaluated by accurate palpation in order to make sure
that the defects have been eliminated and that the two sides are
symmetrical. Meticulous care at this stage of the operation pays
good dividends later, when, after the oedema has gone, the final
result can be appreciated in detail. A few stitches are then
placed to close the marginal incisions .

- In the original Goldman technique, the
dome is cut through completely, dividing cartilage and underlying
soft tissues. In inexpert hands, this complete separation may lead
to complications. Granulation tissue may develop where the dome is
divided, and the resultant scarring can lead to retraction and
irregularities of the tip contour. The completely free crura may
be placed in the wrong position during splinting of the nose or
displaced later. Such displacement may be backwards, forwards,
upwards, or downwards, with consequent deformity of the tip. It
was the risk of these complications that prompted us to modify the
operation and to employ a more conservative technique for the
dome.
-
- We leave the soft tissues underlying the
dome of the alar cartilage intact. The lateral and the medial
crura, freed as described, are supported normally by the soft
tissues, so that displacement and subsequent asymmetry can be
avoided.
- "BUTTERFLY
TIP"
- TECNICA
CHIRURGICA
-
- Prof.
Dott. LIONELLO PONTI
- Negli ultimi anni molti autori hanno
messo in evidenza l'importanza di dare meticolosamente una nuova
forma alle cartilagini alari nella rinoplastica per ottenere un
buon risultato cosmetico e funzionale.
- La tecnica iniziale di Joseph è
stata modificata in vari modi e nuove tecniche vi sono state
aggiunte.
- Molti di queti metodi comportano la
riduzione della larghezza, lunghezza e altezza delle cartilagini
alari tramite la resezione di un segmento lungo il margine
superiore del crus laterale, ed un altro al livello del duomo,
cosicchè la parte resecata prende la foggia
dell'"hokey-stick" .
- L'escissione delle cartilagini alri, se
attuata correttamente, produce un buon rimodellamento della punta
del naso.
- Per molti anni, abbiamo usato la tecnica
di Goldman, che abbiamo modificato per evitare alcuni tranelli. La
riduzione delle cartilagini alari e il rimodellamento della punta
sono completamente differenti nella nostra tecnica.
- La chirurgia della punta è
solitamente la parte più delicata e difficile nella
rinoplastica. Questa tecnica rende il rimodellamento più
semplice e più preciso, cosicchè il risultato
dell'operazione è più facilmente
prevedibile.
-
-
- TECNICA
OPERATORIA
-
- Quando la correzione dei due terzi
superiori del naso è stata completata, viene eseguita un
incisione marginale semicircolare. Questa si estende dal terzo
superiore della columella, lungo il margine inferiore della
cartilagine, all'estremo laterale del crus larterale. Un paio di
forbici leggermente curve viene inserito nell'incisione, un piano
di spaccatura viene individuato sotto il pericondrio e vengono
scalzati i tessuti molli sovrastanti, aprendo le
forbici.
- Lo scalzamento e la dissezione vengono
estesi all'incisione intercartilaginea e in mezzo alle crura
mediali. Una volta che la cartilagine alare è stata
liberata, viene spinta giù con un uncino applicato al
livello del duomo e portato alla vista diretta. Alla giunzione tra
le crura mediali e quelle laterali, è possibile
identificare un incavo che è molto importante per questo
tipo di metodo.
- Un uncino incavato viene posizionato
sotto il duomo per fungere da guida, e la giunzione tra le crura
laterali e mediali viene tagliata da parte a parte, pochi
millimentri lateralmente all'incavo. Questa incisione è
limitata al solo strato cartilagineo: la cute vestibolare
sottostante viene lasciata intatta. Lo stesso procedimento viene
ripetuto sull'altro lato. Le crura mediali vengono agganciate
insieme ed esposte attraverso la narice destra. Queste vengono
tirate e suturate insieme con una sutura da materassaio. Il
piazzamento di questa sutura è estremamente importante
poichè determina la proiezione e la forma della
punta.
- Se le crura mediali non sono ben
allineate, la punta del naso sarà deformata. Ecco
perchè è importante avere un punto di riferimento
per la sutura: questo punto è l'incavo (dent), o
immediatamente sotto, o sopra di esso.
- In questo modo, viene formato un
sostegno dalle crura mediali, sormontato da due piccole ali di
cartilagine corrispondenti a porzioni del duomo.
- La forma di questa struttura porta il
nome di " Butterfly Tip" ( punta a farfalla).
- Una volta che la proiezione e la
lunghezza della punta sono state stabilite, riduciamo la lunghezza
e la larghezza delle crura laterali, se necessario, in modo che
possano combaciare con le crura mediali. Dopo averle poste in
situ, il chirurgo palpa la punta e, se necessario, avanza verso il
margine libero delle crura mediali. Le crura laterali vengono
ridotte tramite l'escissione di un segmento lungo il margine
superiore, e un altro lungo la porzione laterale del
duomo.
- Infine, ogni irregolarità o
difetto residuo viene corretto da resezioni addizionali, come
indicato.
- Prima che il paziente lasci il tavolo
operatorio, la punta viene ricontrollata tramite una accurata
palpazione al fine di assicurarsi che eventuali difetti siano
stati eliminati e che i due lati siano simmetrici. Una meticolosa
attenzione a questo stadio dell'operazione pota vantaggi
successivamente, quando, dopo che l'edema è scomparso, il
risultato finale può essere apprezzato nei dettagli. Pochi
punti vengono posti a chiudere l'incisione marginale.
- Nella tecnica originale di Goldman, il
duomo viene scavato completamente, dividendo la cartilagine e i
sottostanti tessuti molli. In mani inesperte, questa separazione
completa può portare a varie complicazioni.
- La granulazione del tessuto si
può sviluppare dove il duomo viene diviso, e la cicatrice
che ne risulta può portare alla retrazione e ad
irregolarità al profilo della punta. Le crura completamente
libere possono essere poste nella posizione sbagliata durante
l'immmobilizzazione del naso o spostarsi più tardi. Tali
spostamenti possono essere all'indietro, in avanti,
all'insù o all'ingiù, con conseguente deformazione
della punta. Esisteva il rischio di quelle complicazioni che ci
hanno suggerito di modificare l'operazione e di impiegare una
tecnica maggiormente conservativa per il duomo.
- Noi lasciamo intatti i tessuti molli
sottostanti il duomo della cartilagine alare. Le crura laterali e
mediali, liberate come descritto, sono supportate normalmente dai
tessuti molli, in modo che possano essere evitati lo spostamento e
la conseguente asimmetria.
-
- IPPOCRATEIOS
- Mensile
di medicina e chirurgia
- Editrice
SOPI - Roma
- ippocrateios@sopi.it